"I don’t care what you call it," he says. "I care that we get it right."
April 9, 2014 1:15 PM Subscribe
About half of countries who attempt to build single-payer systems fail. That’s Hsiao’s estimate after working with about 10 governments in the past two decades. Whether he’s in Taiwan, Cyprus, or Vermont, the process is roughly the same: meet with legislators, draw up a plan, write legislation. Only half of those bills actually become law. The part where it collapses is, inevitably, when the country has to pay for it.Ezra Klein's Vox Media looks at the financial and administrative mechanics of Governor Peter Shumlin's quest to bring single-payer health care to Vermont. Bonus: 12 questions about single-payer.
I mean, I'm sure there are a lot of people from outside Vermont who travel there and end up visiting one of the state's fine hospitals. Either the hospitals have to retain their billing and coding departments to deal with this, or the state is going to have to take on the billing and basically act as a central department for the whole state.
This has already been solved in other countries where single payer healthcare kicks in. If my wife becomes ill in Australia when we visit, she simply heads to the hospital, we pay the very reasonable MBS fee and then submit it to our insurance company when we get home to be reimbursed in accordance to our out-of-network plan.
I, on the other hand, just flash my Medicare card and get free hospital admission while I'm back home.
posted by Talez at 1:45 PM on April 9, 2014 [2 favorites]
This has already been solved in other countries where single payer healthcare kicks in. If my wife becomes ill in Australia when we visit, she simply heads to the hospital, we pay the very reasonable MBS fee and then submit it to our insurance company when we get home to be reimbursed in accordance to our out-of-network plan.
I, on the other hand, just flash my Medicare card and get free hospital admission while I'm back home.
posted by Talez at 1:45 PM on April 9, 2014 [2 favorites]
Either the hospitals have to retain their billing and coding departments to deal with this
If (going forward) hospitals etc only have to deal with the US insurance paperwork nightmare for one in a hundred patients (ie sick/injured visitors) instead of almost all patients, then the billing departments will be handling a hundred times less paperwork and can presumably downscale, passing along considerable savings even though the wasting of labor has not been eliminated completely.
posted by anonymisc at 1:50 PM on April 9, 2014 [3 favorites]
If (going forward) hospitals etc only have to deal with the US insurance paperwork nightmare for one in a hundred patients (ie sick/injured visitors) instead of almost all patients, then the billing departments will be handling a hundred times less paperwork and can presumably downscale, passing along considerable savings even though the wasting of labor has not been eliminated completely.
posted by anonymisc at 1:50 PM on April 9, 2014 [3 favorites]
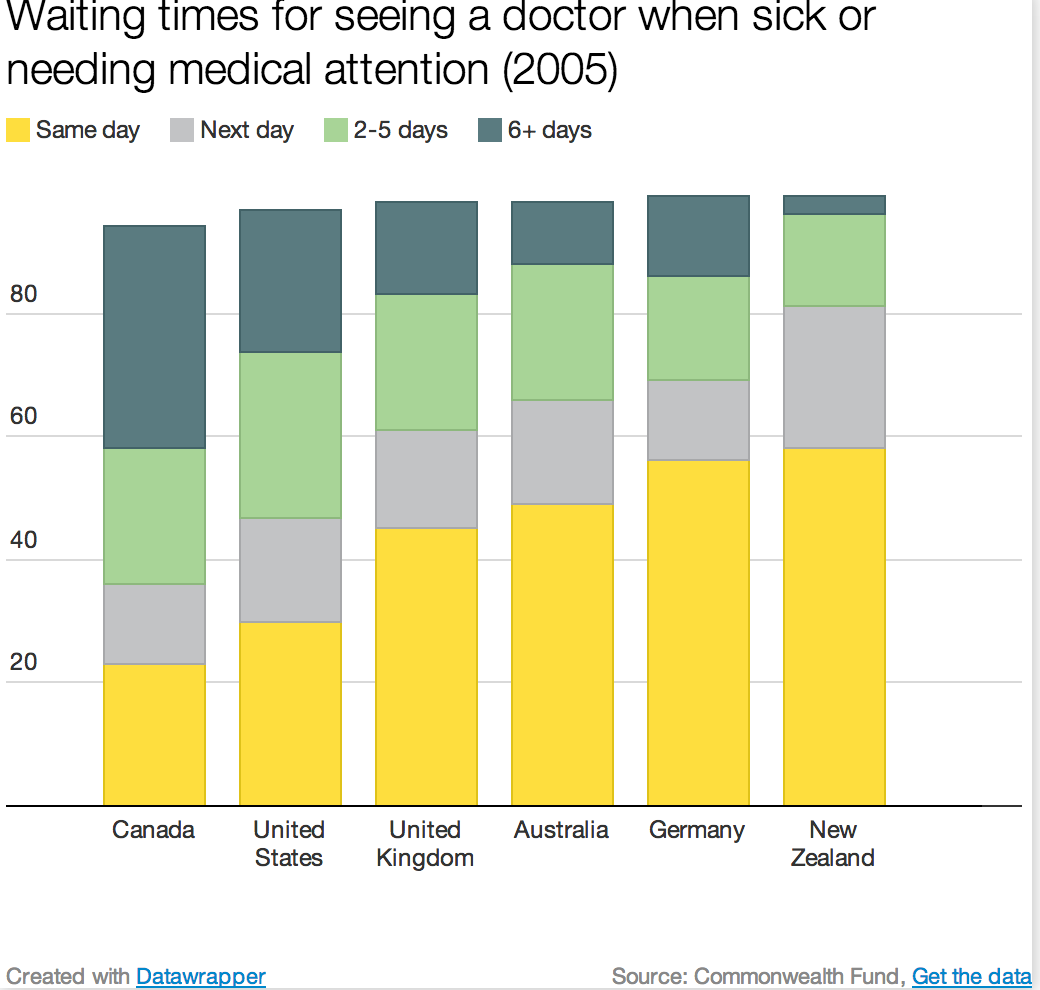
I was surprised by the wait times graph
I knew that the USA wait times didn't seem any shorter than other places I'd been, despite conservative rhetoric claiming otherwise, but I didn't realize that the US system was so far behind even in this one metric where so many people think it shines.
I guess that people only think their shit shines because Canada is the country next door and it manages slightly worse performance. Seen in a wider context however, the US system isn't even managing to do the one thing people assume it's good at (and AFAIK that's even after rigging the score wildly in the US's favor by simply not counting the millions of Americans whose wait times were infinite because they had no healthcare)
posted by anonymisc at 2:01 PM on April 9, 2014 [23 favorites]
{kind=link}
I knew that the USA wait times didn't seem any shorter than other places I'd been, despite conservative rhetoric claiming otherwise, but I didn't realize that the US system was so far behind even in this one metric where so many people think it shines.
I guess that people only think their shit shines because Canada is the country next door and it manages slightly worse performance. Seen in a wider context however, the US system isn't even managing to do the one thing people assume it's good at (and AFAIK that's even after rigging the score wildly in the US's favor by simply not counting the millions of Americans whose wait times were infinite because they had no healthcare)
posted by anonymisc at 2:01 PM on April 9, 2014 [23 favorites]
Also, there's no reason why Vermont can't have it both ways. It's perfectly feasible for the VT legislature to incorporate "Green Mountain Healthcare Inc." and fund it out of an income tax increase. Then give everyone an insurance card. If a company wishes to provide premium health insurance which covers extras then by all means let them do it. If the rich want a hospital with private suites with gold plated fixtures and doctors that drive a Rolls, by all means let them and their privately acquired insurance pay for it.
Meanwhile, Green Mountain Healthcare Inc. agrees to pay the same rate as Medicare and is accepted wherever Medicare is and agrees to fund the public county healthcare systems already in place.
posted by Talez at 2:01 PM on April 9, 2014
Meanwhile, Green Mountain Healthcare Inc. agrees to pay the same rate as Medicare and is accepted wherever Medicare is and agrees to fund the public county healthcare systems already in place.
posted by Talez at 2:01 PM on April 9, 2014
Isn't the problem with doing it both ways that the governor and other proponents of a single-payer system are counting on the savings that would result from a simplified billing and insurance system?
posted by Area Man at 2:05 PM on April 9, 2014
posted by Area Man at 2:05 PM on April 9, 2014
Isn't the problem with doing it both ways that the governor and other proponents of a single-payer system are counting on the savings that would result from a simplified billing and insurance system?
If Australia is any indication, what you find is that about a third to half of people will end up being treated as private patients. Sometimes, the hassle of deductibles can outweigh the advantage of being treated privately. For example when I had my car crash I ended up being treated as a public patient as a public hospital instead of going private simply because I didn't require to skip any sort of wait (it was an ED admission) and because I knew if I went in as a private patient I'd be hit with a deductible plus a gap for whatever treatment I needed. I only needed an x-ray, a tetanus shot and a check for a concussion. Nothing major.
Also, in Australia the claim is submitted and pre-approved straight away. When I went to get my last pair of glasses before I left for the US they took my private health insurance card, swiped it and they immediately had a figure of exactly how much my private insurance would cover and I paid the rest. They had only one person working on administration at any one time despite optical not being covered by Medicare other than the exam itself. It all depends on implementation.
posted by Talez at 2:15 PM on April 9, 2014
If Australia is any indication, what you find is that about a third to half of people will end up being treated as private patients. Sometimes, the hassle of deductibles can outweigh the advantage of being treated privately. For example when I had my car crash I ended up being treated as a public patient as a public hospital instead of going private simply because I didn't require to skip any sort of wait (it was an ED admission) and because I knew if I went in as a private patient I'd be hit with a deductible plus a gap for whatever treatment I needed. I only needed an x-ray, a tetanus shot and a check for a concussion. Nothing major.
Also, in Australia the claim is submitted and pre-approved straight away. When I went to get my last pair of glasses before I left for the US they took my private health insurance card, swiped it and they immediately had a figure of exactly how much my private insurance would cover and I paid the rest. They had only one person working on administration at any one time despite optical not being covered by Medicare other than the exam itself. It all depends on implementation.
posted by Talez at 2:15 PM on April 9, 2014
Also, there's no reason why Vermont can't have it both ways.
If not carefully managed, this'll end with the same problem the public schools are running into -- rich people getting their own privatized system and then systematically defunding the public system. If we are going to have a system of equal access to equal care, there will need to be one system (whether a publicly regulated and facilitated system of private insurance with equalizing subsidies, a la Obamacare and Germany, a publicly funded system with private providers like Ontario, or a publicly funded and managed system such as the UK's NHS).
There can still be opportunities for insurance companies to sell supplemental insurance, extra dental, vision, non-essential coverage, etc. to people who can afford it. But the guy who makes $300K a year must not be allowed to jump the line in front of the guy who makes 30 grand. Upcharge for private suites? Maybe. But no amount of money entitles someone to a better doctor or faster medical care.
posted by tivalasvegas at 2:18 PM on April 9, 2014 [9 favorites]
If not carefully managed, this'll end with the same problem the public schools are running into -- rich people getting their own privatized system and then systematically defunding the public system. If we are going to have a system of equal access to equal care, there will need to be one system (whether a publicly regulated and facilitated system of private insurance with equalizing subsidies, a la Obamacare and Germany, a publicly funded system with private providers like Ontario, or a publicly funded and managed system such as the UK's NHS).
There can still be opportunities for insurance companies to sell supplemental insurance, extra dental, vision, non-essential coverage, etc. to people who can afford it. But the guy who makes $300K a year must not be allowed to jump the line in front of the guy who makes 30 grand. Upcharge for private suites? Maybe. But no amount of money entitles someone to a better doctor or faster medical care.
posted by tivalasvegas at 2:18 PM on April 9, 2014 [9 favorites]
Kadin2048: "But if you're a tourist in the UK and end up in the hospital, at least based on the anecdotal experiences my friends have had, the NHS just eats the cost. "
Yep, and very nicely, and it's very disorienting. I sprained my ankle badly and was freaking out and everyone was all, "Oh, just pop down the street to the surgery and they'll sort you." I barely had to do any paperwork even. Generally if you have to be admitted to the hospital, NHS wants you to pay for it, but if it's routine care, infectious disease, or a minor ER visit that only requires outpatient care, they cover it. And really, the NHS spending 5 minutes wrapping my ankle and getting me sorted out for painkillers and crutches for free was a lot lot faster and cheaper (in terms of staff time overhead) than generating all the paperwork for me that I would have needed to submit it to my insurance company back in the U.S. to pay them.
Kadin2048: "I can't see Vermont doing the latter, or they'd suddenly have a new and very expensive (to Vermont) tourist industry on their hands. "
With taxes, a lot of states that have big neighboring/shared metro areas with a lot of cross-border commuters have an agreement between the two states where they work out between themselves how much tax Illinois residents working in Indiana have had withheld by Indiana, and how much tax Indiana residents working in Illinois have had withheld by Illinois, settle the difference between themselves, with one state remitting an amount to the other, and then employees are allowed to count their withholdings in Indiana towards their Illinois taxes, instead of having to file to have their Indiana withholdings reimbursed to them and then pay the full Illinois amount. (I believe many countries have a similar arrangement for social security programs, where your social-security-paying work years in one country can count as credit in another country, but maybe only for ex-pats intending to return to country of origin.)
If I were Vermont and concerned about out-of-state people getting costly medical care, I'd probably do three things: First, set a cut-off amount at which it makes sense to pursue out-of-state reimbursement -- probably it's easier just to treat someone with strep throat for free, because it's pretty cheap and then they don't infect 30 Vermonters. Second, levy a small "HRA" (hotels, restaurants, and amusements) tax on, well, hotels and ski resorts and so forth, to cover at least some of the cost of tourists receiving routine care for colds and sprained ankles. Third, push neighboring states (New Hampshire, New York) for bilateral agreements at the state government level where you reimburse directly at that level rather than at the individual level, and then New York is responsible for chasing down the individual if they want to. I think the third point would be a hard sell when there's just ONE state with single-payer healthcare, but there are definitely points you can make in its favor (ensures your traveling New York citizens get better health care for cheaper!), and if other states move towards a state-based single-payer model, I as a small state with a large tourist industry would DEFINITELY want direct reimbursement to be part of the conversation. Even though point three is doomed to fail, I want to get it in people's heads as an idea NOW so that it will seem like a sensible solution LATER.
That's just spitballing based on some things states already do in the U.S. to deal with other similar issues, they may or may not be good ideas. I'm sure Canada has a system because their health cards are provincial rather than national; there are definitely models out there to look at.
posted by Eyebrows McGee at 2:27 PM on April 9, 2014 [3 favorites]
Yep, and very nicely, and it's very disorienting. I sprained my ankle badly and was freaking out and everyone was all, "Oh, just pop down the street to the surgery and they'll sort you." I barely had to do any paperwork even. Generally if you have to be admitted to the hospital, NHS wants you to pay for it, but if it's routine care, infectious disease, or a minor ER visit that only requires outpatient care, they cover it. And really, the NHS spending 5 minutes wrapping my ankle and getting me sorted out for painkillers and crutches for free was a lot lot faster and cheaper (in terms of staff time overhead) than generating all the paperwork for me that I would have needed to submit it to my insurance company back in the U.S. to pay them.
Kadin2048: "I can't see Vermont doing the latter, or they'd suddenly have a new and very expensive (to Vermont) tourist industry on their hands. "
With taxes, a lot of states that have big neighboring/shared metro areas with a lot of cross-border commuters have an agreement between the two states where they work out between themselves how much tax Illinois residents working in Indiana have had withheld by Indiana, and how much tax Indiana residents working in Illinois have had withheld by Illinois, settle the difference between themselves, with one state remitting an amount to the other, and then employees are allowed to count their withholdings in Indiana towards their Illinois taxes, instead of having to file to have their Indiana withholdings reimbursed to them and then pay the full Illinois amount. (I believe many countries have a similar arrangement for social security programs, where your social-security-paying work years in one country can count as credit in another country, but maybe only for ex-pats intending to return to country of origin.)
If I were Vermont and concerned about out-of-state people getting costly medical care, I'd probably do three things: First, set a cut-off amount at which it makes sense to pursue out-of-state reimbursement -- probably it's easier just to treat someone with strep throat for free, because it's pretty cheap and then they don't infect 30 Vermonters. Second, levy a small "HRA" (hotels, restaurants, and amusements) tax on, well, hotels and ski resorts and so forth, to cover at least some of the cost of tourists receiving routine care for colds and sprained ankles. Third, push neighboring states (New Hampshire, New York) for bilateral agreements at the state government level where you reimburse directly at that level rather than at the individual level, and then New York is responsible for chasing down the individual if they want to. I think the third point would be a hard sell when there's just ONE state with single-payer healthcare, but there are definitely points you can make in its favor (ensures your traveling New York citizens get better health care for cheaper!), and if other states move towards a state-based single-payer model, I as a small state with a large tourist industry would DEFINITELY want direct reimbursement to be part of the conversation. Even though point three is doomed to fail, I want to get it in people's heads as an idea NOW so that it will seem like a sensible solution LATER.
That's just spitballing based on some things states already do in the U.S. to deal with other similar issues, they may or may not be good ideas. I'm sure Canada has a system because their health cards are provincial rather than national; there are definitely models out there to look at.
posted by Eyebrows McGee at 2:27 PM on April 9, 2014 [3 favorites]
Most of the time out-of-province care is covered by reciprocal billing, as in your example. You do have to be careful though, there can be holes in coverage.
posted by bonehead at 2:42 PM on April 9, 2014
posted by bonehead at 2:42 PM on April 9, 2014
Third, push neighboring states (New Hampshire, New York) for bilateral agreements at the state government level where you reimburse directly at that level rather than at the individual level, and then New York is responsible for chasing down the individual if they want to.
Maybe New York would go for it, but I think it would be a very cold day in hell before New Hampshire agreed to anything like that, just on general principle. What's in it for them, exactly?
posted by Kadin2048 at 2:43 PM on April 9, 2014 [1 favorite]
Maybe New York would go for it, but I think it would be a very cold day in hell before New Hampshire agreed to anything like that, just on general principle. What's in it for them, exactly?
posted by Kadin2048 at 2:43 PM on April 9, 2014 [1 favorite]
The reason health cost administration is such a big thing in the USA is specifically because the hospitals are being run as a business and they're negotiating different deals with different insurance companies. If Vermont's government establishes a schedule of payments for different procedures then all that goes out the window: the hospital, which is now getting 80% (90%? whatever) of its income from the government has a firm basis for rejecting any deal that pays less, and the insurance companies won't want to pay more. So basically the only difference is that the hospital or the patient needs to submit a standard bill with standard pricing, rather than attempt to fit their procedure into yet another arcane reimbursement formula.
posted by Joe in Australia at 2:46 PM on April 9, 2014 [1 favorite]
posted by Joe in Australia at 2:46 PM on April 9, 2014 [1 favorite]
I think it's great that Vermont is trying to find a proper solution to the administration of health care, but this article is both extremely, patently biased against single-payer and not very helpful in making sense of the reported claims. Here are a few examples of what I mean:
1. The administrative savings of a single-payer system do come at a price. Single payer requires the government to make difficult decisions about what benefits they will and won’t cover — and often leave out pretty standard medical services, things like prescription drugs or dentist visits.
This is incredibly misleading. Single payer requires the adoption of certain standards, but this makes it sound like other systems don't also involve difficult decision-making, which they do. So this isn't really a "price" of single payer so much as a feature of absolutely any and every health care system which has to allocate finite resources, and likewise, other systems also leave things out completely, including dentist visits.
2. Single-payer countries are often associated with longer wait times, a perception that stems from Canada’s system.
So, not really a fact so much as a perception, which like any is susceptible to manipulation by, oh I don't know, people who are profiting obscenely from the current market system and their armies of lobbyists perhaps.
3. Vermont wasn’t satisfied with the health reform law that Washington passed in 2010, the Affordable Care Act. That law expands health coverage by growing the existing health-care system.
I hate this kind of dopey equivocation. The ACA builds on the current system and doesn't change the fundamental mechanism of the private market, but it doesn't "grow" anything: programs cost money and require administration and oversight, and there's no free sunlight or soil for them to draw upon. Society is not a garden. Things like "the economy" or health-care system don't grow, they interact with everything else in specific and often complex ways.
4. Between now and then there are two big questions that Vermont has to answer: how much will single-payer cost, and can the state find a way to pay for it?
Can individuals find ways to pay for their health care right now? Can everyone else pay the high price of uncontrolled medical costs? The current system is greatly improved by the ACA, but Americans are still overpaying for health care by an absurd degree for absolutely no good reason. Talking about single-payer as though the system already in place doesn't already cost people way too much money is just shamelessly disingenuous.
5. The Shumlin administration contracted with London and a team of economists last year to estimate the cost of Vermont’s plan. Their report estimates that Vermont will need to raise an additional $1.6 billion in tax revenue in 2017 to pay for a single-payer system...In the Vermont legislature, most people ballpark the cost of single-payer somewhere around $2 billion — and spend even more time worrying about how to raise that money.
This isn't a false claim, exactly, but once again they throw that huge figure out there without bothering to find out how much (for instance) the state and private citizens are already overpaying as a consequence of having privatized health care that enables great latitude in gouging and profiteering. Again, the choices about which facts to report can't be mistaken for good faith.
6. Vermont isn’t alone in its money problems. Single-payer countries around the world have regularly struggled with figuring out the best way to pay for the system.
And yet again, the authors characterize payment as a problematic issue that governments have to deal with when they're paying, but one that private citizens apparently don't have to worry about when health care comes out of our pockets.
7. About half of countries who attempt to build single-payer systems fail.
This is probably the most inflammatory and obnoxious part of the whole article. It's an incredibly tendentious way of saying that institutional political failures prevent citizens from getting what they deserve, which we already know.
None of these seven things are outright falsehoods, but each is a subtle manipulation (and some are not at all subtle) that distorts reality to greater or lesser degrees, and that's especially odious when the subject of the article is so regularly and constantly misrepresented for political reasons already.
posted by clockzero at 2:50 PM on April 9, 2014 [29 favorites]
1. The administrative savings of a single-payer system do come at a price. Single payer requires the government to make difficult decisions about what benefits they will and won’t cover — and often leave out pretty standard medical services, things like prescription drugs or dentist visits.
This is incredibly misleading. Single payer requires the adoption of certain standards, but this makes it sound like other systems don't also involve difficult decision-making, which they do. So this isn't really a "price" of single payer so much as a feature of absolutely any and every health care system which has to allocate finite resources, and likewise, other systems also leave things out completely, including dentist visits.
2. Single-payer countries are often associated with longer wait times, a perception that stems from Canada’s system.
So, not really a fact so much as a perception, which like any is susceptible to manipulation by, oh I don't know, people who are profiting obscenely from the current market system and their armies of lobbyists perhaps.
3. Vermont wasn’t satisfied with the health reform law that Washington passed in 2010, the Affordable Care Act. That law expands health coverage by growing the existing health-care system.
I hate this kind of dopey equivocation. The ACA builds on the current system and doesn't change the fundamental mechanism of the private market, but it doesn't "grow" anything: programs cost money and require administration and oversight, and there's no free sunlight or soil for them to draw upon. Society is not a garden. Things like "the economy" or health-care system don't grow, they interact with everything else in specific and often complex ways.
4. Between now and then there are two big questions that Vermont has to answer: how much will single-payer cost, and can the state find a way to pay for it?
Can individuals find ways to pay for their health care right now? Can everyone else pay the high price of uncontrolled medical costs? The current system is greatly improved by the ACA, but Americans are still overpaying for health care by an absurd degree for absolutely no good reason. Talking about single-payer as though the system already in place doesn't already cost people way too much money is just shamelessly disingenuous.
5. The Shumlin administration contracted with London and a team of economists last year to estimate the cost of Vermont’s plan. Their report estimates that Vermont will need to raise an additional $1.6 billion in tax revenue in 2017 to pay for a single-payer system...In the Vermont legislature, most people ballpark the cost of single-payer somewhere around $2 billion — and spend even more time worrying about how to raise that money.
This isn't a false claim, exactly, but once again they throw that huge figure out there without bothering to find out how much (for instance) the state and private citizens are already overpaying as a consequence of having privatized health care that enables great latitude in gouging and profiteering. Again, the choices about which facts to report can't be mistaken for good faith.
6. Vermont isn’t alone in its money problems. Single-payer countries around the world have regularly struggled with figuring out the best way to pay for the system.
And yet again, the authors characterize payment as a problematic issue that governments have to deal with when they're paying, but one that private citizens apparently don't have to worry about when health care comes out of our pockets.
7. About half of countries who attempt to build single-payer systems fail.
This is probably the most inflammatory and obnoxious part of the whole article. It's an incredibly tendentious way of saying that institutional political failures prevent citizens from getting what they deserve, which we already know.
None of these seven things are outright falsehoods, but each is a subtle manipulation (and some are not at all subtle) that distorts reality to greater or lesser degrees, and that's especially odious when the subject of the article is so regularly and constantly misrepresented for political reasons already.
posted by clockzero at 2:50 PM on April 9, 2014 [29 favorites]
And yet again, the authors characterize payment as a problematic issue that governments have to deal with when they're paying, but one that private citizens apparently don't have to worry about when health care comes out of our pockets.
I'm in favor of Vermont creating a single-payer system, but I think you are wrong to be too dismissive of the political challenges involved in raising taxes in Vermont to the point that there is $2 billion more state revenue. Sure, you can tell people that this will all work out because they mostly won't be paying for health care any more, and I think that's broadly true, but that argument isn't guaranteed to make political resistance to substantial tax increases disappear.
It is important to remember that some portion of the cost of the current system is being paid by employers. Once Green Mountain Healthcare is implemented, that money won't automatically transfer into salary or wages. So, a person could see their payroll tax increase significantly and not see an increase in their pay to cover that tax increase. That's the sort of thing that can anger voters, and the Governor of Vermont has to get this plan through an elected legislature. I think this political challenge can be solved, but just hand-waving it away isn't productive.
posted by Area Man at 3:12 PM on April 9, 2014 [2 favorites]
I'm in favor of Vermont creating a single-payer system, but I think you are wrong to be too dismissive of the political challenges involved in raising taxes in Vermont to the point that there is $2 billion more state revenue. Sure, you can tell people that this will all work out because they mostly won't be paying for health care any more, and I think that's broadly true, but that argument isn't guaranteed to make political resistance to substantial tax increases disappear.
It is important to remember that some portion of the cost of the current system is being paid by employers. Once Green Mountain Healthcare is implemented, that money won't automatically transfer into salary or wages. So, a person could see their payroll tax increase significantly and not see an increase in their pay to cover that tax increase. That's the sort of thing that can anger voters, and the Governor of Vermont has to get this plan through an elected legislature. I think this political challenge can be solved, but just hand-waving it away isn't productive.
posted by Area Man at 3:12 PM on April 9, 2014 [2 favorites]
If not carefully managed, this'll end with the same problem the public schools are running into -- rich people getting their own privatized system and then systematically defunding the public system.
I get the feeling, though, that once people experience single-payer care, they'll see to it that their elected representatives prioritize its careful management. Which is exactly why single-payer scares the shit out of Republican (and some Democratic) politicians--they don't want to lose elections over opposing it.
On top of that, health care is way more relevant to a larger block of voters (i.e., over-50s) than public schools are, so I suspect those voters would fight attempts to defund public health care the way schools have been. Of course, it was those over-50s who bought into the smaller-government bullshit in the first place way back when, so that might be wishful thinking on my part. But it seems logical given how much the average person would benefit, in real-world, not-choosing-between-medicine-and-food terms, from single-payer.
But no amount of money entitles someone to a better doctor or faster medical care.
Why do you hate America?
posted by Rykey at 3:29 PM on April 9, 2014
I get the feeling, though, that once people experience single-payer care, they'll see to it that their elected representatives prioritize its careful management. Which is exactly why single-payer scares the shit out of Republican (and some Democratic) politicians--they don't want to lose elections over opposing it.
On top of that, health care is way more relevant to a larger block of voters (i.e., over-50s) than public schools are, so I suspect those voters would fight attempts to defund public health care the way schools have been. Of course, it was those over-50s who bought into the smaller-government bullshit in the first place way back when, so that might be wishful thinking on my part. But it seems logical given how much the average person would benefit, in real-world, not-choosing-between-medicine-and-food terms, from single-payer.
But no amount of money entitles someone to a better doctor or faster medical care.
Why do you hate America?
posted by Rykey at 3:29 PM on April 9, 2014
That’s Hsiao’s estimate after working with about 10 governments in the past two decades.
"About 10 governments"? What a bizarre way to write, if you want your reader to believe you.
posted by Ice Cream Socialist at 3:38 PM on April 9, 2014 [6 favorites]
"About 10 governments"? What a bizarre way to write, if you want your reader to believe you.
posted by Ice Cream Socialist at 3:38 PM on April 9, 2014 [6 favorites]
I'm in favor of Vermont creating a single-payer system, but I think you are wrong to be too dismissive of the political challenges involved in raising taxes in Vermont to the point that there is $2 billion more state revenue.
I think you're inadvertently attributing to me a position I do not hold. To clarify, I was talking about the explanatory style of the article and arguing that it's very biased, which is exemplified in the fact that the authors regard one kind of expenditure (what the state would pay, with a single payer plan) as worth reporting while apparently not realizing or not caring that the money that is already spent on health care is also a cost which can be calculated and is relevant to the situation.
Sure, you can tell people that this will all work out because they mostly won't be paying for health care any more, and I think that's broadly true, but that argument isn't guaranteed to make political resistance to substantial tax increases disappear.
You have to distinguish between political resistance and the technical feasibility of a program. The former is not a reliable indicator of anything factual.
It is important to remember that some portion of the cost of the current system is being paid by employers. Once Green Mountain Healthcare is implemented, that money won't automatically transfer into salary or wages.
Why shouldn't it be transferred, actually? Why not make that a provision of the program? Companies are already parting with that money, why not improve the standard of living by just having it go into people's paychecks? Then it could be taxed like the rest of their income to support the plan, too.
So, a person could see their payroll tax increase significantly and not see an increase in their pay to cover that tax increase. That's the sort of thing that can anger voters, and the Governor of Vermont has to get this plan through an elected legislature. I think this political challenge can be solved, but just hand-waving it away isn't productive.
That could happen, under the condition that the law would be written that way, or things could happen differently. And since I wasn't really addressing the issue of how to structure this program anyway, I don't really see your point being especially applicable to what I was saying. You can talk about whatever you want to, of course, but other people aren't wrong simply because they aren't talking about the same thing.
posted by clockzero at 3:39 PM on April 9, 2014 [2 favorites]
I think you're inadvertently attributing to me a position I do not hold. To clarify, I was talking about the explanatory style of the article and arguing that it's very biased, which is exemplified in the fact that the authors regard one kind of expenditure (what the state would pay, with a single payer plan) as worth reporting while apparently not realizing or not caring that the money that is already spent on health care is also a cost which can be calculated and is relevant to the situation.
Sure, you can tell people that this will all work out because they mostly won't be paying for health care any more, and I think that's broadly true, but that argument isn't guaranteed to make political resistance to substantial tax increases disappear.
You have to distinguish between political resistance and the technical feasibility of a program. The former is not a reliable indicator of anything factual.
It is important to remember that some portion of the cost of the current system is being paid by employers. Once Green Mountain Healthcare is implemented, that money won't automatically transfer into salary or wages.
Why shouldn't it be transferred, actually? Why not make that a provision of the program? Companies are already parting with that money, why not improve the standard of living by just having it go into people's paychecks? Then it could be taxed like the rest of their income to support the plan, too.
So, a person could see their payroll tax increase significantly and not see an increase in their pay to cover that tax increase. That's the sort of thing that can anger voters, and the Governor of Vermont has to get this plan through an elected legislature. I think this political challenge can be solved, but just hand-waving it away isn't productive.
That could happen, under the condition that the law would be written that way, or things could happen differently. And since I wasn't really addressing the issue of how to structure this program anyway, I don't really see your point being especially applicable to what I was saying. You can talk about whatever you want to, of course, but other people aren't wrong simply because they aren't talking about the same thing.
posted by clockzero at 3:39 PM on April 9, 2014 [2 favorites]
Vermont has to double its tax revenues to do it. I'll believe that when I see it.
posted by jpe at 4:30 PM on April 9, 2014
posted by jpe at 4:30 PM on April 9, 2014
On top of that, health care is way more relevant to a larger block of voters (i.e., over-50s)
Medicare age voters already get a great deal through the feds. You expect them to swallow a 2x tax hike to pay for younger generations?
posted by jpe at 4:33 PM on April 9, 2014
Medicare age voters already get a great deal through the feds. You expect them to swallow a 2x tax hike to pay for younger generations?
posted by jpe at 4:33 PM on April 9, 2014
Not all countries do it the same. Check out this PBS doc from a few years back.
In Switzerland (at the time of the doc), insurance companies were basically forced to become non-profits. They can sell supplementary insurance but essentially the compete for the government reimbursements.
posted by MiltonRandKalman at 4:41 PM on April 9, 2014
In Switzerland (at the time of the doc), insurance companies were basically forced to become non-profits. They can sell supplementary insurance but essentially the compete for the government reimbursements.
posted by MiltonRandKalman at 4:41 PM on April 9, 2014
And what about medicaid recipients? They'll pay higher sales taxes for something they already get free?
posted by jpe at 4:49 PM on April 9, 2014
posted by jpe at 4:49 PM on April 9, 2014
Sure, you can tell people that this will all work out because they mostly won't be paying for health care any more, and I think that's broadly true, but that argument isn't guaranteed to make political resistance to substantial tax increases disappear.
The United States spends $8000 per head on health care and doesn't cover everyone.
Canada spends $5500 per head and covers everyone.
Other countries do better than Canada. Since there is less money per head, that means there is a smaller portion of GDP being devoted to a basic necessity, which is good for the country as a whole, and for individual tax payers who end up paying the bill either way. Single payer health care isn't possible in the United States because it would reduce profits, and profits for private corporations are more important than keeping our citizens healthy and alive.
posted by deanklear at 5:55 PM on April 9, 2014 [6 favorites]
The United States spends $8000 per head on health care and doesn't cover everyone.
Canada spends $5500 per head and covers everyone.
Other countries do better than Canada. Since there is less money per head, that means there is a smaller portion of GDP being devoted to a basic necessity, which is good for the country as a whole, and for individual tax payers who end up paying the bill either way. Single payer health care isn't possible in the United States because it would reduce profits, and profits for private corporations are more important than keeping our citizens healthy and alive.
posted by deanklear at 5:55 PM on April 9, 2014 [6 favorites]
Two paragraphs stuck out to me, in a "these are linked" kind of way.
The first one, starting with: "In 1947, Saskatchewan began doing something very different from the rest of the country: it decided to pay the hospital bills for all residents. The system was popular and effective — and other provinces quickly took notice."
And the one that starts with: "Vermont’s doctors and hospitals are skeptical of this estimate — and generally protest the idea that the single-payer system will lead to administrative savings."
Why? Because the first paragraph ignores that when, in the 60s, Saskatchewan went from hospitals to universal health care (bringing doctors under the act, essentially), the doctors went on strike in order to shut down health care. For almost a month. The government brought in scab doctors from out-of-province to break them.
Of course, nowadays most doctors will acknowledge that medicare is better to have than not have, ignoring the edge problems.
So forgive me if I am less than trusting of the Vermont doctors' skepticism.
posted by Lemurrhea at 6:36 PM on April 9, 2014 [4 favorites]
The first one, starting with: "In 1947, Saskatchewan began doing something very different from the rest of the country: it decided to pay the hospital bills for all residents. The system was popular and effective — and other provinces quickly took notice."
And the one that starts with: "Vermont’s doctors and hospitals are skeptical of this estimate — and generally protest the idea that the single-payer system will lead to administrative savings."
Why? Because the first paragraph ignores that when, in the 60s, Saskatchewan went from hospitals to universal health care (bringing doctors under the act, essentially), the doctors went on strike in order to shut down health care. For almost a month. The government brought in scab doctors from out-of-province to break them.
Of course, nowadays most doctors will acknowledge that medicare is better to have than not have, ignoring the edge problems.
So forgive me if I am less than trusting of the Vermont doctors' skepticism.
posted by Lemurrhea at 6:36 PM on April 9, 2014 [4 favorites]
Canadian healthcare isn't perfect, true, but you know what? As an American who married a Canadian and moved up here, I will freakin' take it. I forgot what it was like to be able to not have to worry about going to a doctor or a dentist (not covered) without having to worry about can I make rent this month? What can I eat if because I am gonna give the majority of my food budget to making sure my cats will be okay?
I could not do these things as an American living in Atlanta working on just above minimum wage. I had to hope nothing went wrong.
Canadians (and I guess, by proxy, me now) pay fairly high taxes because this system covers everyone. Sure, there will always be bitching and complaining about "freeloaders," but I feel that Canada does less to poor-shame than my home country.
My husband had a fairly unpleasant American healthcare incident in 2012 when we vacationed in the US. In fact, you can read it about it here. To follow up, despite the fact he was fully covered by our travel insurance, we are still getting calls from that place demanding the full amount of his bill. Our Canadian insurer is at a loss because the American company demanding the amount will not call them to confirm the account.
posted by Kitteh at 6:41 PM on April 9, 2014 [1 favorite]
I could not do these things as an American living in Atlanta working on just above minimum wage. I had to hope nothing went wrong.
Canadians (and I guess, by proxy, me now) pay fairly high taxes because this system covers everyone. Sure, there will always be bitching and complaining about "freeloaders," but I feel that Canada does less to poor-shame than my home country.
My husband had a fairly unpleasant American healthcare incident in 2012 when we vacationed in the US. In fact, you can read it about it here. To follow up, despite the fact he was fully covered by our travel insurance, we are still getting calls from that place demanding the full amount of his bill. Our Canadian insurer is at a loss because the American company demanding the amount will not call them to confirm the account.
posted by Kitteh at 6:41 PM on April 9, 2014 [1 favorite]
The United States spends $8000 per head on health care and doesn't cover everyone.
Not only does the US pay way more than any other country for healthcare - its heathcare outcomes are decidedly middling.
Or, to put it another way - if the political will was there, the US could halve its spending on healthcare, while greatly improving outcomes for its entire population.
posted by HiroProtagonist at 6:51 PM on April 9, 2014 [1 favorite]
Not only does the US pay way more than any other country for healthcare - its heathcare outcomes are decidedly middling.
Or, to put it another way - if the political will was there, the US could halve its spending on healthcare, while greatly improving outcomes for its entire population.
posted by HiroProtagonist at 6:51 PM on April 9, 2014 [1 favorite]
Canadians (and I guess, by proxy, me now) pay fairly high taxes because this system covers everyone.
New Zealand has lower taxes than the USA, and a universal healthcare system that is better than Canada's one (according to various graphs in the link).
You're not paying high taxes to cover everyone. You're just paying high taxes. :-/
posted by anonymisc at 6:54 PM on April 9, 2014 [3 favorites]
New Zealand has lower taxes than the USA, and a universal healthcare system that is better than Canada's one (according to various graphs in the link).
You're not paying high taxes to cover everyone. You're just paying high taxes. :-/
posted by anonymisc at 6:54 PM on April 9, 2014 [3 favorites]
But the guy who makes $300K a year must not be allowed to jump the line in front of the guy who makes 30 grand
That. Will. Be. The. Day.
If you make $300K or better, you can just buy your own damn line and screw those freeloaders.
posted by BlueHorse at 6:55 PM on April 9, 2014 [1 favorite]
That. Will. Be. The. Day.
If you make $300K or better, you can just buy your own damn line and screw those freeloaders.
posted by BlueHorse at 6:55 PM on April 9, 2014 [1 favorite]
The situation of out-of-state visitors to VT hospitals is mentioned. What about the other way around? I know a lot of people in my neck of the woods who have gone to Dartmouth for procedures and emergencies.
posted by MtDewd at 7:23 PM on April 9, 2014
posted by MtDewd at 7:23 PM on April 9, 2014
> Medicare age voters already get a great deal through the feds. You expect them to swallow a 2x tax hike to pay for younger generations?
How many people of Medicare age pay payroll tax?
> And what about medicaid recipients?
How many people on Medicaid pay much in payroll taxes?
Payroll taxes for the major portion of funds makes the most sense because their employers are currently paying for their healthcare. The payroll tax just replaces the employer health insurance premiums. Eliminate a cap and more money comes from high-income people. That is the way Medicare works.
posted by JackFlash at 10:57 PM on April 9, 2014
How many people of Medicare age pay payroll tax?
> And what about medicaid recipients?
How many people on Medicaid pay much in payroll taxes?
Payroll taxes for the major portion of funds makes the most sense because their employers are currently paying for their healthcare. The payroll tax just replaces the employer health insurance premiums. Eliminate a cap and more money comes from high-income people. That is the way Medicare works.
posted by JackFlash at 10:57 PM on April 9, 2014
Payroll taxes are literally a tax on jobs and fail to hit people whose income comes from investments. Income and sales taxes don't have this problem. I take your point about payroll taxes replacing employer contributions, but this is actually a good reason to make the switch: single-payer health care funded by income and sales tax would make labor cheaper, and reduce unemployment.
posted by Joe in Australia at 12:34 AM on April 10, 2014
posted by Joe in Australia at 12:34 AM on April 10, 2014
I was surprised by the wait times graphAs they also point out later, it's even worse than that in the US: people who can't afford healthcare and thus stay away from medical institutions are not counted in the statistics but effectively have an infinite wait time. Including those - as they would automatically be in a system with universal coverage - would make the wait time statistic even worse.
I knew that the USA wait times didn't seem any shorter than other places I'd been, despite conservative rhetoric claiming otherwise, but I didn't realize that the US system was so far behind even in this one metric where so many people think it shines.
posted by brokkr at 2:16 AM on April 10, 2014 [1 favorite]
Payroll taxes are literally a tax on jobs and fail to hit people whose income comes from investments.
Stocks and Bonds are real property that are bought and sold. So... Simply assessing sales and property taxes solves both State ( sales ) and Local ( property ) revenue issues quite nicely.
posted by mikelieman at 2:24 AM on April 10, 2014
Stocks and Bonds are real property that are bought and sold. So... Simply assessing sales and property taxes solves both State ( sales ) and Local ( property ) revenue issues quite nicely.
posted by mikelieman at 2:24 AM on April 10, 2014
"About 10 governments"? What a bizarre way to write, if you want your reader to believe you.
Mmm, I dunno. Hsiao's clearly an expert in the field and this sort of consulting isn't a discrete process. There may have been a couple of one-off meetings among the more-involved advisory gigs.
posted by psoas at 4:14 AM on April 10, 2014
Mmm, I dunno. Hsiao's clearly an expert in the field and this sort of consulting isn't a discrete process. There may have been a couple of one-off meetings among the more-involved advisory gigs.
posted by psoas at 4:14 AM on April 10, 2014
So forgive me if I am less than trusting of the Vermont doctors' skepticism.
Indeed. For what it's worth, the Vermont doctors I know (my aunt and uncle, who both work at a regional hospital in Randolph) are both enthusiastically pro-single-payer, and their coworkers are apparently similarly enthusiastic. So there's your competing anecdata, anyway.
posted by Mayor West at 5:31 AM on April 10, 2014
Indeed. For what it's worth, the Vermont doctors I know (my aunt and uncle, who both work at a regional hospital in Randolph) are both enthusiastically pro-single-payer, and their coworkers are apparently similarly enthusiastic. So there's your competing anecdata, anyway.
posted by Mayor West at 5:31 AM on April 10, 2014
Mmm, I dunno. Hsiao's clearly an expert in the field and this sort of consulting isn't a discrete process. There may have been a couple of one-off meetings among the more-involved advisory gigs.
Yes, and that's the kind of thing a good writer or interviewer would clarify. Since ten is a small number, "about" adds shade. Where precision is impossible, explaining why sheds light.
Otherwise some readers are left thinking, Forty is "about 50." So is zero "about ten?"
posted by Ice Cream Socialist at 7:18 AM on April 10, 2014
Yes, and that's the kind of thing a good writer or interviewer would clarify. Since ten is a small number, "about" adds shade. Where precision is impossible, explaining why sheds light.
Otherwise some readers are left thinking, Forty is "about 50." So is zero "about ten?"
posted by Ice Cream Socialist at 7:18 AM on April 10, 2014
Stocks and Bonds are real property that are bought and sold. So... Simply assessing sales and property taxes solves both State ( sales ) and Local ( property ) revenue issues quite nicely.
Stocks and bonds are not "real property", they're "personal property". Specifically, they're intangible personal property, which Vermont doesn't tax. AFAICT, Vermont doesn't tax personal property at a state level at all, and some municipalities tax business personal property but not that of individuals. So that's not a revenue stream that they have access to currently, and it would be a pretty significant change to their tax structure — and probably not a popular one — to suddenly institute it.
Again, keep in mind that the governor's mandate wasn't exactly huge. It's not clear that he has the political capital to push through significant tax changes like that.
Florida used to have one as a way mostly of hitting retirees with lots of assets but no income, but it was repealed a few years ago, except on mortgages. I've never run into it elsewhere. Washington State seems to be playing with the idea of taxing businesses on intangibles, including goodwill, which would be interesting.
posted by Kadin2048 at 9:00 AM on April 10, 2014
Stocks and bonds are not "real property", they're "personal property". Specifically, they're intangible personal property, which Vermont doesn't tax. AFAICT, Vermont doesn't tax personal property at a state level at all, and some municipalities tax business personal property but not that of individuals. So that's not a revenue stream that they have access to currently, and it would be a pretty significant change to their tax structure — and probably not a popular one — to suddenly institute it.
Again, keep in mind that the governor's mandate wasn't exactly huge. It's not clear that he has the political capital to push through significant tax changes like that.
Florida used to have one as a way mostly of hitting retirees with lots of assets but no income, but it was repealed a few years ago, except on mortgages. I've never run into it elsewhere. Washington State seems to be playing with the idea of taxing businesses on intangibles, including goodwill, which would be interesting.
posted by Kadin2048 at 9:00 AM on April 10, 2014
Yep, and very nicely, and it's very disorienting. I sprained my ankle badly and was freaking out and everyone was all, "Oh, just pop down the street to the surgery and they'll sort you." I barely had to do any paperwork even. Generally if you have to be admitted to the hospital, NHS wants you to pay for it, but if it's routine care, infectious disease, or a minor ER visit that only requires outpatient care, they cover it. And really, the NHS spending 5 minutes wrapping my ankle and getting me sorted out for painkillers and crutches for free was a lot lot faster and cheaper (in terms of staff time overhead) than generating all the paperwork for me that I would have needed to submit it to my insurance company back in the U.S. to pay them.
Part of this is philosophical, part of it's pragmatic. Unless you've had something major done to you it's normally cheaper for the NHS to eat the cost of the procedure than pay for a specialist insurance wrangler to try to get the money out of a US insurance company. And that's without taking into account the fact that our doctors wouldn't even think to ask what your insurance will cover (saving everyone a lot of time and the doctors a lot of bureaucracy where time is most needed) and the medical notes are written to a standard where they will tell doctors what happened rather than to a standard where they will provide no wriggle room for the insurance companies to argue. We are used to billing once to cover the entire hospital spell and (other than in very complex cases) at no point does the doctor have to worry about the costs or anything other than the best practice treatment available.
And I really must write that blog post explaining how NHS billing works and how to get approximate values for the income a hospital receives from a hospital stay.
posted by Francis at 3:37 PM on April 10, 2014
Part of this is philosophical, part of it's pragmatic. Unless you've had something major done to you it's normally cheaper for the NHS to eat the cost of the procedure than pay for a specialist insurance wrangler to try to get the money out of a US insurance company. And that's without taking into account the fact that our doctors wouldn't even think to ask what your insurance will cover (saving everyone a lot of time and the doctors a lot of bureaucracy where time is most needed) and the medical notes are written to a standard where they will tell doctors what happened rather than to a standard where they will provide no wriggle room for the insurance companies to argue. We are used to billing once to cover the entire hospital spell and (other than in very complex cases) at no point does the doctor have to worry about the costs or anything other than the best practice treatment available.
And I really must write that blog post explaining how NHS billing works and how to get approximate values for the income a hospital receives from a hospital stay.
posted by Francis at 3:37 PM on April 10, 2014
« Older 100 Best Hoosier albums ever | He is tremendously tall and has a wonderful... Newer »
This thread has been archived and is closed to new comments
I mean, I'm sure there are a lot of people from outside Vermont who travel there and end up visiting one of the state's fine hospitals. (Skiing and hospitalization pretty much go hand and hand, in my mind. I'm also not a very good skiier.) Either the hospitals have to retain their billing and coding departments to deal with this, or the state is going to have to take on the billing and basically act as a central department for the whole state. The latter seems significantly more efficient — let all the non-resident bills roll up to one office at the state level, and deal with the insurance companies from there — but I don't know if you could legally do it unless the state owns the hospitals themselves.
Internationally, I believe that if you are a non-resident not covered by the national health program in Canada, you have to pay for your services upfront and then handle getting reimbursed from your own insurance company on your own time (and dime). But if you're a tourist in the UK and end up in the hospital, at least based on the anecdotal experiences my friends have had, the NHS just eats the cost.
I can't see Vermont doing the latter, or they'd suddenly have a new and very expensive (to Vermont) tourist industry on their hands. But maybe they could do the former? Just tell VT hospitals that they don't have to deal with out-of-state insurance companies anymore, and thus they become "out of network" pay-or-go-straight-to-collections for everyone besides Vermonters? That would seem to be the simplest solution.
posted by Kadin2048 at 1:38 PM on April 9, 2014